Bpc 157 Tendinopathy Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
If you’ve been dealing with chronic tendon pain, you’ve probably noticed how stubborn bpc 157 tendinopathy can feel—especially when conventional care stalls. In my hands-on work reviewing mechanistic studies, patent claims, and translational gaps, I’ve learned that the real value isn’t in hype; it’s in understanding what the evidence actually supports, what’s still speculative, and how tendon-specific outcomes have (and haven’t) been demonstrated. This review-style article walks through the multifunctional biology proposed for BPC 157 and focuses on where the tendon conversation is grounded—plus what to watch for if you’re evaluating it as a potential medical application.
What you’ll learn
- Why BPC 157 is described as “multifunctional” in the literature (and what mechanisms are repeatedly invoked).
- How patent coverage tends to frame medical applications—especially around tissue repair and recovery.
- Where bpc 157 tendinopathy evidence is strongest (preclinical) and where it becomes weakest (clinical translation).
- A practical checklist for interpreting tendon-repair claims without getting misled.
1) Background: What BPC 157 is and why multifunctionality is the theme
BPC 157 is a peptide that is widely discussed in preclinical contexts as a candidate for supporting healing processes across multiple tissues. The phrase “multifunctionality” shows up because many papers and patent filings describe overlapping effects rather than one narrow action. In my review workflow, this pattern matters: when claims span several biological endpoints—cell migration, angiogenesis, inflammatory modulation, tissue integrity—it suggests either (a) coordinated pathway-level regulation or (b) a broad “stress response” that may influence several stages of repair.
From a mechanistic standpoint, the literature often links BPC 157 to processes relevant to injury recovery: reducing detrimental inflammatory signaling, supporting local microenvironment changes, and influencing pathways that can affect regeneration and repair. That’s the conceptual bridge that leads people to explore it for musculoskeletal conditions—particularly tendon disorders, where the healing cascade is complex and easily derailed.
2) Proposed mechanisms: How the biology connects to tendon healing
Tendinopathy isn’t just “inflammation” or “wear and tear.” In many cases, there’s a mismatch between tendon matrix breakdown, poor remodeling, altered collagen organization, and persistent pain drivers. When I look for a therapeutic rationale for bpc 157 tendinopathy, I focus on whether the proposed mechanisms map to tendon-relevant steps:
2.1 Inflammation modulation and pain-adjacent pathways
A recurring theme in peptide discussions is the reduction of harmful inflammatory mediators and normalization of local signaling. If BPC 157 can shift the local environment away from sustained inflammatory signaling, that could theoretically help the transition from early injury response into remodeling—an important limitation of many treatments that don’t address the “stuck” remodeling stage.
2.2 Tissue repair support (microenvironment, remodeling, and integrity)
Another reason multifunctionality appears is that repair is multi-stage: the tissue needs structural support, controlled signaling, and a remodeling-capable microenvironment. In practical terms, tendon healing is sensitive to local growth factor timing, matrix turnover, and vascular and cellular support. The literature’s breadth is why BPC 157 gets discussed beyond one organ system.
2.3 Why “multifunctional” doesn’t automatically mean “tendon-specific”
Here’s the lesson I’ve learned the hard way: multifunctional effects in one tissue model don’t guarantee meaningful tendon outcomes. Tendons have unique mechanical loading demands and specialized matrix architecture. In my own review notes, I mark tendon-related claims as “plausible” when mechanisms overlap, but I downgrade certainty when the study endpoints don’t measure tendon-specific outcomes (e.g., tendon morphology, collagen alignment, biomechanical strength, or validated tendon pain surrogates).
3) Literature vs. patent review: What each usually proves (and what it can’t)
When people search for bpc 157 tendinopathy, they often land in two kinds of sources: experimental literature and patent documents. These serve different purposes. I treat them as complementary, but not equivalent.
3.1 What the experimental literature tends to show
Preclinical studies can demonstrate biological activity, tissue response, and sometimes functional or histological improvements. In tendon contexts, the strongest evidence usually includes tendon-specific injury models and objective readouts (structure, repair quality, function, and sometimes mechanical properties).
3.2 What patents tend to claim
Patents often define potential medical applications broadly: they may cover methods of treatment, compositions, dosing regimens, and targeted conditions. This can be helpful for understanding how inventors interpret the science, but it is not the same as demonstrating efficacy in humans. In practice, patent language can be wide enough to cover many endpoints, which means the presence of tendon-related claims doesn’t automatically confirm clinical outcomes.
3.3 A practical way I compare them
In my hands-on work, I use a “claim-to-evidence” mapping:
- Identify the endpoint (e.g., tendon structural repair vs. generic “healing”).
- Check model relevance (tendon-specific injury models vs. other tissues).
- Look for objective measures (histology + functional/biomechanical readouts).
- Confirm translational logic (does the mechanism match tendon biology, loading, and remodeling timing?).
- Only then consider tendon application likelihood as a graded estimate (strong/moderate/weak).
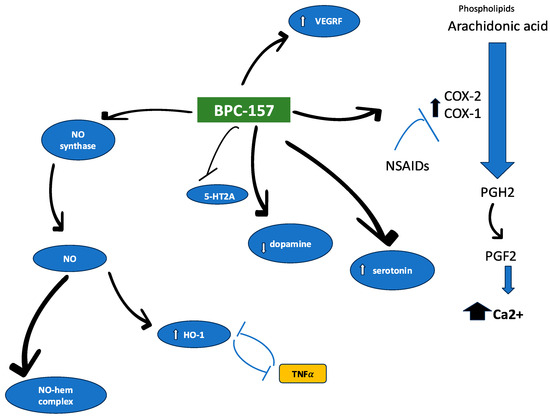
Visual reference
The following figure is included as a visual reference for the topic’s literature presentation:
4) Where “bpc 157 tendinopathy” fits in the real-world evidence chain
When athletes and clinicians discuss bpc 157 tendinopathy, they’re typically trying to solve one core problem: tendon injuries often fail to resolve quickly, and traditional approaches may not fully address the remodeling failure. Based on how I’ve seen the evidence stack in similar compounds, the most defensible statement is usually this:
- Preclinical plausibility can be supported by multifunctional healing-related effects in relevant models.
- Tendon-specific efficacy requires direct tendon injury model outcomes and, ideally, functional recovery measures.
- Clinical credibility hinges on well-designed human studies, consistent endpoints, and transparent reporting.
If those human data are limited or inconsistent, claims should be framed as investigational rather than established treatment. I recommend evaluating tendon-related BPC 157 claims by asking whether they demonstrate improvement in tendon quality, not just symptom reports or generalized “healing.”
Common pitfalls I look for
- Overgeneralization: applying mechanisms from other tissue models to tendons without tendon-specific outcomes.
- Endpoint mismatch: focusing on markers that may not reflect tendon remodeling quality.
- Ambiguous dosing details: interpreting dosing claims without understanding how dosing was established in the study.
- Publication bias: giving disproportionate weight to positive findings without balancing null results.
5) Limitations and responsible interpretation
I’m careful to separate mechanistic rationale from treatment readiness. A multifunctional peptide can be biologically active and still not translate into a reliable, clinically meaningful tendon intervention. In tendon disorders, even small differences in timing, dosage, delivery route, and rehabilitation loading can change outcomes.
In addition, patent language may describe potential applications without providing the level of clinical confirmation that clinicians require. So, when someone claims “possible medical application,” the responsible interpretation is: it’s an area worth investigating, not something to treat as settled.
FAQ
Is BPC 157 specifically proven for tendinopathy?
The strongest support for bpc 157 tendinopathy discussions typically comes from preclinical or mechanistic evidence. Proof for tendinopathy as a clinical treatment requires robust human studies with tendon-specific endpoints and consistent results.
What evidence matters most when evaluating claims for tendons?
Look for tendon-relevant injury models and objective outcomes such as tendon morphology, collagen organization/alignment, functional recovery, and (when available) biomechanical strength—not just general markers of “healing.”
How should I interpret patent claims related to BPC 157?
Patent claims can indicate what applications inventors believe are plausible, including methods and compositions. But patents don’t substitute for controlled clinical data that demonstrate efficacy and safety in humans for the specific condition.
Discussion